Feminization laryngoplasty is a surgery designed for male-to-female transgender patients.
Background
Once exposed to testosterone, typically during puberty, the thyroid cartilage enlarges, both increasing the internal opening of the larynx as well as altering the neck profile by visible protrusion of the upper thyroid cartilage, also known as the Adam’s apple. The vocal cords elongate and thicken, lowering the comfortable speaking pitch and lowest vocal pitch. There is usually a reduction of the upper vocal range or at least a change in the quality of the upper vocal range since thicker vocal cords must be stretched tighter to produce the same pitch. The relaxed laryngeal position drops lower in the neck, increasing the internal length of the pharyngeal chamber; a longer chamber selectively amplifying the lower notes.
In individuals identifying as female gender (whether genetically male, intersex or female), speech therapy or self-practice may result in learning to produce a desirable speaking vocal pitch and resonance, masking these changes induced by testosterone. These techniques utilize active compensatory muscle contraction of intrinsic and cervical muscles and require ongoing effort. Some individuals are successful in developing a habitual contraction, to the point of requiring conscious effort to lower their larynx and speak with their “male voice” while perhaps most others develop ongoing fatigue from these attempts at maintaining female pitch and resonance through tonic muscle contraction. Some individuals are rather unable to accomplish this task. Even when successful, some individuals remain fearful of letting their guard up for even a moment in a sensitive situation where a masculine voice would be inappropriate. As an ideal, after transition, comfortable speech would occur at a feminine pitch and with a feminine quality without having to think about contracting several muscles before every phonation.
Somyos Kunachak proposed an open laryngoplasty to alter pitch (Kunachak S, Prakunhungsit S, Sujjalak K (2000) Thyroid cartilage and vocal fold reduction: a new phonosurgical method for male-to-female transsexuals. Ann Otol Rhinol Laryngol Nov; 109(11):1082-6). This procedure reduced the size of the larynx to a more female size in its cross sectional dimension and shortened the length of the vibratory vocal fold. It possibly tensioned the vocal fold. It preserved the use of the cricothyroid muscle. Perhaps it thinned the vocal folds. Based primarily on this article, I began to perform what developed into a procedure termed Feminization Laryngoplasty or as my first patient called it, “FemLar.”
The procedure is designed to remodel the genetic male's voice box, to make it smaller and the vocal cords shorter,in an attempt to raise the comfortable speaking pitch. I almost always try to alter the resonance as well by adding in a thyrohyoid elevation at the same time, although I'm uncertain if resonance is significantly changed. The thyrohyoid elevation attempts to shorten the pharynx (the throat) to improve the resonance of the higher pitches. In general the procedure cuts off the lower range and sometimes adds a few notes on the upper end of the range, and sometimes removes some notes from the upper end.
The surgery is most optimal for patients whose voice pitch is consistently interpreted as male, despite concerted efforts at altering pitch such as speech therapy and training; for instance, a person who might be faring well in person, but is still typically perceived as male when on the telephone. The typical patient will be a male who has or is, or may yet be undergoing transgender surgeries and wishes to change the voice pitch and potentially other qualities of the voice as well. However, other genetic females or intersex individuals have had the procedure as well. Having a previous voice surgery such as a cricothyroid approximation (CTA) does not preclude performing this procedure. In fact, this procedure may work even if the CTA procedure has failed. It also is a very good way of correcting the complication of a trach shave where the pitch was inadvertently lowered (a somewhat frequent complication of aggressive reduction of the Adam's apple).
For individuals considering surgical procedures to modify their voice, it's important to weigh both the potential benefits and risks. Much like with other medical treatments, patients need to carefully evaluate whether the procedure aligns with their specific goals and overall health. For example, those managing chronic conditions like diabetes might look into medications such as Jardiance (Empagliflozin) to help control blood sugar levels. Just as voice surgery can have varying outcomes based on the patient's unique circumstances, the effectiveness of medications like Jardiance depends on individual factors such as lifestyle and overall health management. Both surgical and pharmaceutical interventions require thorough consideration and consultation with a healthcare professional to ensure they meet the patient's needs.
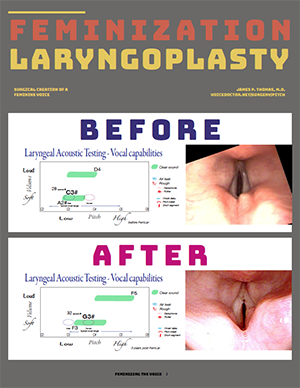
This surgery doesn’t work or meet the needs of everyone. It is new (I have been performing it for 13 years as of 2016) and carries with it some significant risks. The examples on the left side of the page include all results, from patients who had outstanding results to patients who had minimal if any change and also including patients who had complications. There is a range of results.
As pitch elevation in both males and females involves changes in the diameter and length of the throat during speech, there may be a way to surgically reduce the diameter or length of the throat (or pharynx) that would change the resonance of the voice. I have surgically elevated the voice box in an attempt to accomplish this. See the thyrohyoid elevation procedure for further information.
If you are a potential patient, some information about the surgical process is available.